AI Clinical Documentation: How Indian Hospitals Are Reclaiming 2–3 Hours Per Clinician
Inside the AI scribing wave reshaping Indian hospitals — what the technology does, the evidence base, and how to deploy it safely.
A senior physician at a leading Mumbai hospital recently confided: "I spend more time writing about patient care than actually delivering it." This is not an isolated frustration. Across India's hospitals — from Apollo's 70-facility network to district-level clinics — documentation burden has become one of the single largest threats to clinician satisfaction, patient throughput, and care quality.
In 2026, AI-powered clinical documentation is no longer experimental. It is being deployed at scale, validated in real-world settings, and increasingly mandated by accreditation frameworks. This article examines the state of the technology, the Indian context, the evidence base, and what hospital leadership needs to know to implement it safely.
The Documentation Burden: A Crisis Hidden in Plain Sight
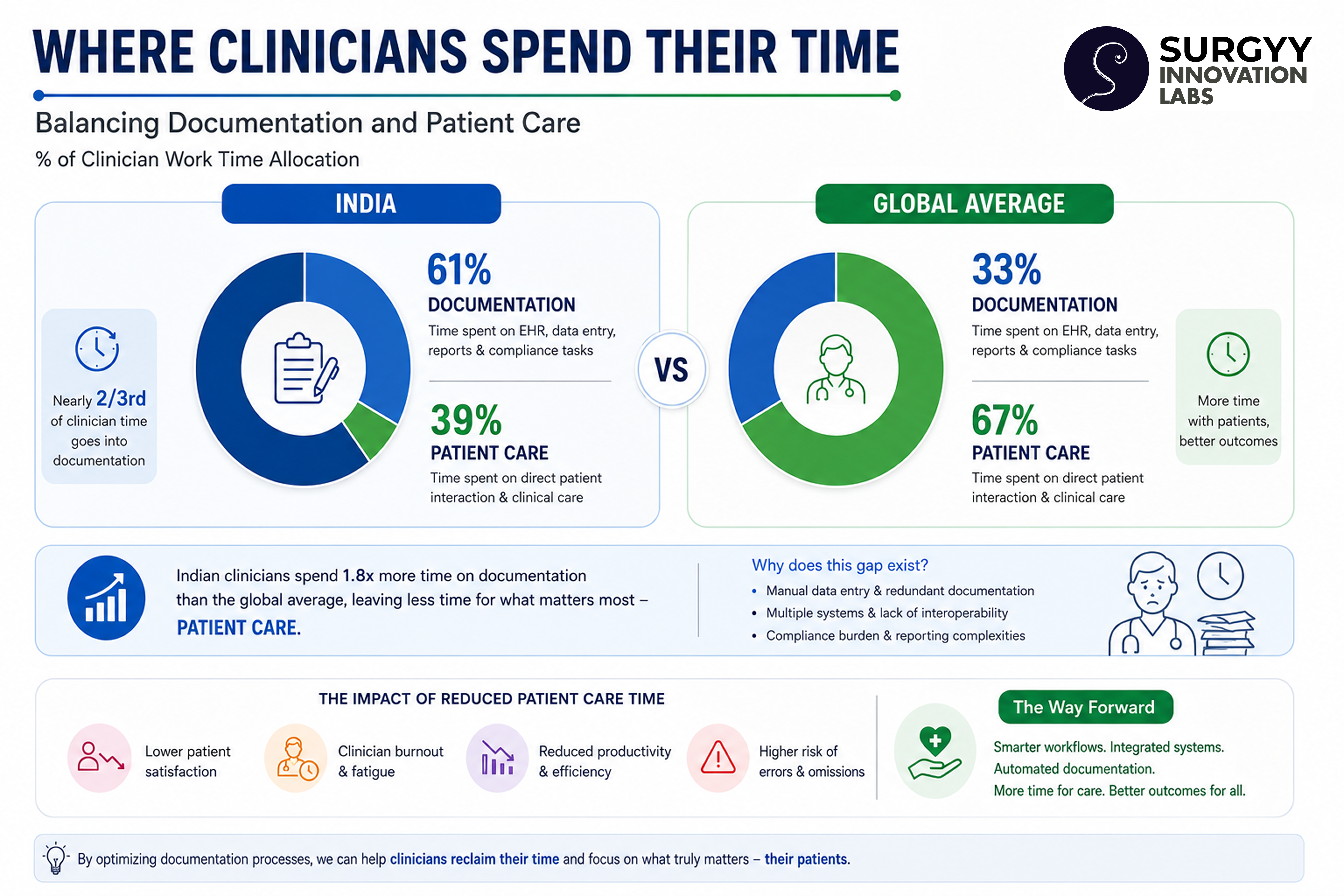
Apollo Hospitals announced in March 2025 that it would direct 3.5% of its digital budget to AI integration, with the specific goal of automating all routine clinical documentation. The arithmetic is straightforward: if a consultant sees 40 patients a day and spends 4–5 minutes documenting each encounter, that is over 3 hours — time that cannot be spent on patient interaction, procedure, or rest.
The consequences ripple outward. Rushed notes lead to incomplete records, which create audit failures, insurance claim rejections, medication errors, and discontinuity of care. Manual discharge summaries — written at the end of exhausting shifts — are one of the most common sources of clinical error at care transitions.
What AI Clinical Documentation Actually Does
The term 'AI documentation' encompasses a range of technologies. Understanding which layer addresses which problem is essential for procurement decisions.
1. Ambient Speech-to-Text (AI Scribing)
The foundational layer: the system listens to the clinician–patient conversation and generates structured clinical notes in real time. Products in this category use large language models fine-tuned on medical dialogue to differentiate chief complaint from history, examination findings from assessment, and plan from instructions. The clinician reviews and edits — the AI drafts.
2. Discharge Summary Automation
Discharge summaries are the bête noire of hospital documentation — long, complex, time-sensitive, and frequently incomplete. AI systems now pull structured data from the Electronic Health Record (diagnosis codes, medications, vitals, lab trends) and generate a first-pass discharge summary that the clinician refines. This is the most measurable ROI use case for hospitals with existing HIS/EHR infrastructure.
3. Pre-built Clinical Templates
Specialty-specific templates — OPD notes for nephrology, orthopaedics, cardiology; ICU progress notes; pre-anaesthesia assessments — dramatically reduce blank-page burden. AI systems auto-populate structured fields from dictation or previous records.
4. Multilingual Documentation
India's linguistic diversity creates a unique challenge absent in Western markets. A clinician in Tamil Nadu may examine a patient in Tamil and need to document in English. AI systems with multilingual support — including transliteration and code-switching — are a critical capability for Indian deployments.
"AI triage algorithms route patients to appropriate care tiers — reducing unnecessary emergency presentations by an estimated 22%." — India's AI Healthcare Strategy 2026, SAHI Framework
The Indian Market Context: Why Now?
Three converging factors have made 2025–26 the inflection point for AI documentation in India:
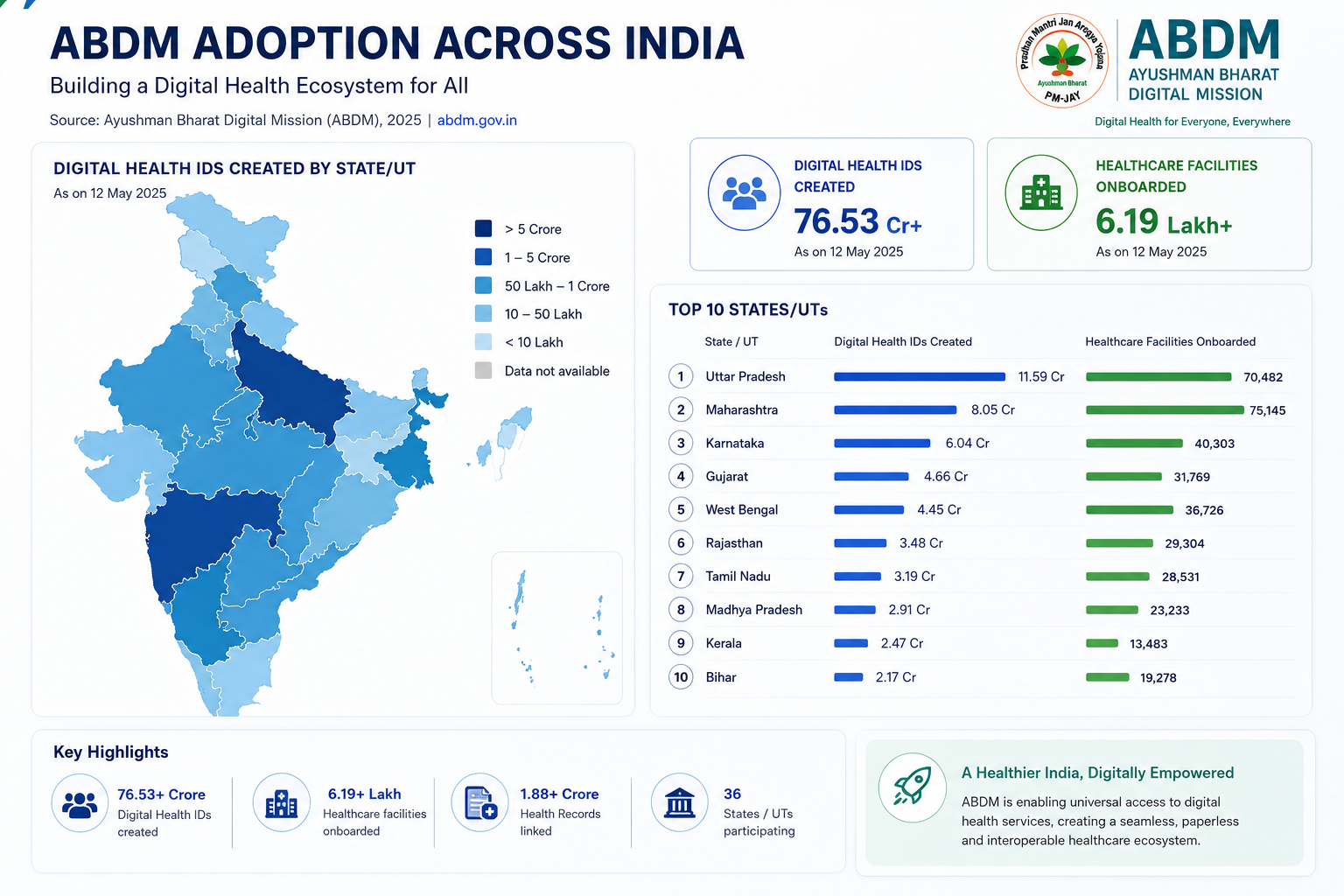
- ABDM Infrastructure: The Ayushman Bharat Digital Mission has created 799 million digital health IDs and linked 671 million health records. As hospitals migrate to ABDM-compliant HIS platforms, the data substrate for AI documentation becomes available at scale.
- NABH 6th Edition Digital Mandate: The requirement to digitally track 75% of patient records has accelerated HIS adoption. AI documentation tools integrate naturally with this infrastructure. See our NABH 6th Edition roadmap.
- Physician Attrition Pressure: India faces a ratio of 0.74 physicians per 1,000 population — well below the WHO recommended 1.0. Reducing documentation burden is one of the few levers available to increase effective clinician capacity without training new doctors.
Evidence: Does It Actually Work?
The evidence base is growing rapidly. Key findings from recent deployments:
- AI-driven OCR can transcribe doctors' handwritten notes and printed forms into digital records with high reliability, reducing transcription errors significantly (Daily Pioneer, January 2026).
- Apollo's AI documentation pilots showed potential to save 2–3 hours per clinician per day.
- AI Clinical Decision Support Systems on eSanjeevani have assisted 12 million telemedicine consultations with diagnostic recommendations.
- A KPMG–FICCI 2025 report positioned AI documentation as a key lever for India's ambition to become the world's healthcare capital.
Critically, the evidence also highlights risks. A 2026 Wolters Kluwer report warned of 'clinical deskilling' — the risk that clinicians who over-rely on AI-generated notes may lose the narrative reasoning skills embedded in manual documentation. Governance frameworks that keep clinicians in the review loop are essential.
SurgyScribe: AI Clinical Documentation Built for Indian Hospitals
Surgyy's SurgyScribe is designed from the ground up for the Indian clinical environment. Key capabilities:
- Live transcription with real-time structuring into clinical note formats
- Pre-built templates for OPD, discharge summaries, referrals, and specialist notes
- Mobile-friendly — start a note on mobile, complete on desktop, without data loss
- Multilingual support for India's diverse clinical settings
- Clean, minimalist interface optimised for rapid clinician review and edit
Deployed across hospitals ranging from single-specialty clinics to multi-facility networks, SurgyScribe integrates with existing HIS/EHR systems without requiring infrastructure replacement.
Implementation Considerations for Hospital Leadership
1. Start with Discharge Summaries
The highest ROI and most measurable impact. Pilot with one ward, measure time-to-discharge-summary and completeness scores, then scale.
2. Establish a Governance Protocol
AI-generated notes must be reviewed, edited, and signed by a licensed clinician before they enter the legal medical record. Define this workflow explicitly. The clinician remains medically and legally responsible.
3. Train Staff Before Deployment
Change management is underestimated in clinical AI deployment. Clinicians need to understand what the AI can and cannot do. A structured onboarding programme — delivered via an LMS — significantly accelerates adoption.
4. Integrate with NABH Documentation Requirements
Map your AI documentation outputs to NABH Chapter 9 (IMS) requirements. Ensure digital records meet the 75% threshold mandated by the 6th Edition.
The Road Ahead: From Documentation to Decision Support
AI documentation is the gateway drug to a broader clinical AI ecosystem. Once structured, searchable patient records exist at scale, the next layer — predictive analytics, clinical decision support, early warning systems — becomes possible. India's SAHI framework targets AI deployment across diagnostics, disease surveillance, maternal health, cancer screening, and chronic disease management.
For hospital leaders, the message is clear: investing in AI documentation infrastructure today is not just an operational efficiency play. It is the foundational investment that makes every subsequent clinical AI application possible.
References
- Apollo Hospitals AI Documentation Plans — Daily Pioneer, January 2026
- Wolters Kluwer: 2026 Healthcare AI Trends
- KPMG–FICCI: AI in Healthcare India, October 2025
- ARC Advisory: AI in Healthcare India 2026
- India AI Healthcare Strategy — SAHI Framework 2026
- Surgyy SurgyScribe — AI Clinical Documentation — surgyy.com

Written by
Mohammed Jamil Nasir
Founder — Product & Tech, Surgyy Innovation Labs
12+ years in Product, Design & Tech · PGC AI/ML, IIT-Guwahati · Global MBA, SP Jain · BE-CSE
Mohammed Jamil Nasir leads product and technology at Surgyy Innovation Labs, building AI tools for India's hospitals and healthcare networks. He writes about healthcare AI, accreditation, and clinical operations.
Connect on LinkedInKeep reading

Why Hospitals Need More Than a CRM: How SurgyCRM Closes the Gap Between Patient Acquisition and Lifetime Value
SurgyCRM is the only healthcare-native CRM that unifies patient acquisition, clinical journey management, feedback, and field sales into one AI-powered platform — purpose-built for hospitals in India and the GCC.

NABH 6th Edition: Your Complete 2026 Roadmap to Hospital Accreditation in India
Standards, digital mandates, costs, timelines and a 12-month plan to get your hospital NABH-accredited under the new 6th Edition.